An Interview between Harrison Lancaster MD and Justin Hartupee MD PhD FACC
Edited by Mustafa Husaini MD MBA FACC
- We often think of a heart failure patient’s hemodynamic profile according to the 2×2 wet vs dry & cold vs wet. Can you discuss why this is important, both for patients in the ICU and on the floor, and how you determine which bucket to place a patient in?
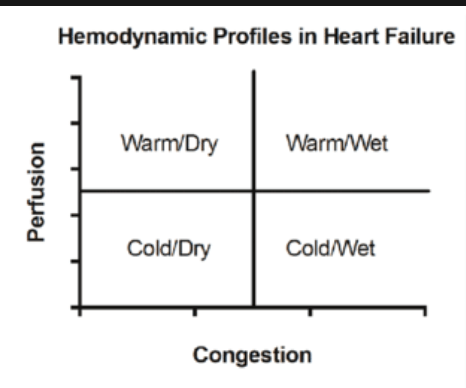
When you are initially evaluating a patient with heart failure, using these hemodynamic profiles can be a good place to start. In the 2×2 method, you are trying to categorize patients based on perfusion and congestion. On the congestion axis, you can categorize patients as “wet” or “dry”. On the perfusion axis, you can categorize patients as “warm” or “cold”. The vast majority of patients who are admitted to the hospital are going to be in the “warm and wet” category, which means they are volume overloaded but don’t have signs of malperfusion.
To assess for congestion, you can use a combination of history and physical to place patients into their respective categories. If a patient is complaining of worsening shortness of breath, lower extremity edema , orthopnea, or PND, then I would categorize that patients as “wet”. Be careful with broad generalizations though, because there are tons of things that can cause a patient to feel short of breath; thus, dyspnea alone may not necessarily mean a patient is congested or having an exacerbation of their heart failure. Obviously on exam, if you see edema, JVD, or abdominal distention that fits the “wet” profile as well.
When assessing for perfusion, your physical exam and laboratory testing are usually the most useful in determining where a patient may fall. You will obviously want to feel their lower extremities to see if they are warm or cold. Typically, I associated an elevated lactate as a more specific test for poor perfusion. Other lab values that could be indicative of poor perfusion and end organ dysfunction would be elevated liver function tests or creatinine. Although, in reality these lab abnormalities would rarely be due to true poor perfusion and are more likely from congestion (congestive hepatopathy, cardiorenal syndrome). True poor perfusion from heart failure (Cardiogenic shock) is uncommon, but obviously it is important to catch early so those patients can quickly get the care they need.
So, I do think this is a useful way to think about patients that can help you determine how sick they are and what medicines you would want to give them. I also think it is important, however, to understand the limitations of this tool. Use this method with the understanding that clinical syndromes other than heart failure can cause congestion and poor perfusion, but this is a good place to start.
Once we understand where our patients are in terms of these classification systems, we can start to think about managing their hemodynamics to improve their clinical condition. Let’s break this down into specific hemodynamic components.
- Before we get into specific hemodynamic components, do you have any advice for residents who are hoping to improve their ability to assess a patient’s hemodynamic status?
I think understanding and assessing a patient’s hemodynamics is like everything else in life, it takes practice. I think something that can be very helpful is trying to estimate hemodynamics for patients who are going to get a formal assessment in the cath lab, and then understanding why your estimations were accurate or not. It is important to understand that you won’t always be perfect. I have been doing this for a while now and still have patients where I can’t determine their volume status. So, practice as much as you can with the patients you are taking care of and ask your attending when you aren’t sure.
Preload:
- What is preload and when is it high, low, or normal? What is the mechanism by which preload optimization improves cardiac function?
Preload is really ventricular filling or more specifically, ventricular stretch. At its purest, preload represent a volume. Unfortunately, we do not have good ways to measure volume, so we use pressure as an estimate for the volume that represents preload. This is with the understanding that this is an imperfect estimate, as pressure and volume are not perfectly correlated. Typically, these pressures are measured with a right heart catheterization. The values we would use would be a right atrial pressure, left atrial or pulmonary capillary wedge pressure, and left ventricular end diastolic volume. These pressures can give you an estimation of ventricular filling, or “preload”.
When preload is low, I think of volume loss. Some clinical examples that come to mind would be GI bleeding, sepsis, or a diarrheal illness. Preload is high when there is too much volume. This is what we see most often with patients with heart failure who present with signs of congestion like we discussed earlier.
Why optimizing preload is important really comes down to the Frank Starling curve mechanism. This curve shows that as preload goes up, cardiac output or stroke volume also goes up due to the increased stretch on ventricular myocytes. So obviously, increasing preload can improve cardiac output for patients who are volume down (1 -> 2). However, there is a point of diminishing returns, where as you go up in volume, you are not going to get anymore increase in cardiac output, and can start driving symptoms of congestion or high intra-cardiac filling pressures (2 -> 3). This is why we diuresis to reduce preload, to try and get back to the ideal part of the starling curve (3 -> 2)

- What are conditions where we consider a patient’s clinical symptoms as a “pump” problem, rather than an “input” problem (fluid)?
I think using an example may best answer your question. Let’s say you have a patient who presents with congestion, so you try and diurese them to optimize their preload. However, this patient does not diurese very well and starts to develop worsening renal dysfunction and/or their lactate starts going up. Then you are confused and wondering if the patient is truly not congested and you are taking away too much of their preload. Or, is there something else going on that is driving the problem. This is a scenario where the patient may benefit from going to the cath lab and having their hemodynamics clarified with a right heart catheterization. These patients may have severely depressed ventricular contractility (I.E., a “pump” problem), and may need inotropic support in addition to preload optimization.
In these scenarios, you make an initial assessment of a patient’s volume status, then start to backtrack when your treatments aren’t working in the way you would expect. The example above is probably what we see most in the realm of Cardiology. We occasionally think patients are volume overloaded, but when taken to the cath lab, they actually have low-normal intra-cardiac filling pressures and lower cardiac output.
On the other end of the spectrum, sometimes patients will present with overt volume loss from a GI bleed or sepsis, but don’t get better with adequate volume resuscitation. Then you may have an issue with contractility or some other mechanism driving the clinical picture, just as above.
I think the biggest teaching point here is that; you should make an initial assessment of a patient’s hemodynamic and volume status, then when things aren’t going the way you would expect, consider getting more data to clarify the hemodynamics. This is clinical reasoning, thinking why the outcome was different than you had anticipated and then reconciling the delta.
- How do we think about preload differently in patients with RV dysfunction or pulmonary hypertension?
When we are thinking about some of these conditions, you will want to sort out which patients are “preload dependent”. RV failure and pulmonary arterial hypertension are some classic clinical conditions that we think of this way. In these patients, you don’t want to diurese them too much. “Preload dependent” means that these patients need the preload to generate enough cardiac output to overcome the resistance working against the ventricle. So, we worry about diuresing these patient’s too much, but at the same time you can’t let these patients get too congested either. So in these patients I would think a little more carefully about their volume status so you don’t accidentally get too aggressive with diuresis and send them into shock.
When you are thinking about a patient with pulmonary hypertension, then you really want to know why they have pulmonary hypertension. Patient’s with pulmonary arterial hypertension and patient’s with pulmonary hypertension from elevated left sided cardiac filling pressures behave differently.
Patients who have pulmonary hypertension because they have elevated left sided filling pressures, this is less of a “preload dependent” condition. In these patients, diuresing them will decrease their pulmonary pressure and help improve their hemodynamics. Thus, I think understanding if a patient is “preload dependent” is important to consider, however, know that even these patient’s usually need aggressive diuresis also.
Afterload:
- What is afterload and when is it high, low, or normal?
Afterload can be conceptualized as the forces that resist cardiac output or the ejection of blood from the left ventricle. I think of it as the force the heart has to work against to generate cardiac output.
Afterload is typically high in the setting of heart failure. Patients with heart failure have a neurohormonal adaptation to the chronic decrease in cardiac output, which causes an increase in the systemic vascular resistance or “afterload”. Other high afterload conditions would be systemic hypertension or aortic stenosis. In these conditions, a chronically high afterload can actually cause detrimental cardiac remodeling and lead to heart failure.
Some clinical syndromes where afterload is typically low would be sepsis or cirrhosis. Another scenario that comes to mind would be following cardiac surgery, where patients can get vasoplegic. These conditions are all characterized by a very low systemic vascular resistance, which means the pressure the heart is beating against is low.
- What is the mechanism by which afterload reduction improves cardiac function?

- So let’s say we are taking care of a patient on Cardiology firm with Heart Failure – what agents would you typically use to reduce afterload?
When you are taking care of patients on the floor, you are going to want to get them on the medications you want them to be on long term. The ACE/ARB/ARNI group of medications would be the primary afterload reducers in the context of the core components of heart failure therapy (GDMT). These medications all have been shown to reduce mortality, reduced hospitalizations, and control symptoms. These medications are typically where I would start. If there is concern for acute or chronic kidney injury, we often start hydralazine +/- nitrates to achieve afterload reduction.
The MRA medications, such as spironolactone, also play a role in afterload reduction. Typically, when I am taking care of heart failure patients on the floor, the ACE/ARB/ARNI and MRA are the first two classes of medications I start for this reason. These medicines will provide short term hemodynamic benefits while in the hospital, but will also provide those long term mortality benefits as well.

For patients with HFpEF (see image to the right), an important consideration is to treat their hypertension but be cautious with afterload reduction when normotensive. The reason is that patients with HFpEF have exaggerated changes in blood pressure for the same change in afterload (Figure A & C) or preload (Figure B & D) [Borlaug BA. 2011 Mar;32(6):670-9]
- What about an ICU patient?
It is a little bit different in the ICU. If a patient is in cardiogenic shock, then you will want to reduce their afterload with something that is more rapid acting and easily titratable. In terms of oral options, Captopril is usually the best option and can be titrated fairly quickly in the CCU with the help of the nursing staff. Hydralazine and Isordil are other oral options that are fast acting and can be used in these patients. I will say that if a patient is stable enough for oral medications and were previously on Entresto, then I would prefer that Entresto be used over these options because, in my opinion, it is the best medication we have for patients with Heart Failure. There are situations, however, where hydralazine and isordil are preferred in the short term due to renal dysfunction or electrolyte abnormalities that may prevent you from using an ACE/ARB/ARNI.
For patients who are very sick, you will want to use IV medicines to reduce their afterload. The most commonly used medicine for this situation would be Nitroprusside (or “nipride”), which is an arterial and venous vasodilator which works very quickly. This medicine is typically titrated with a Swan Ganz Catheter in place so you can monitor the patient’s hemodynamics very closely, as patients often do have a rapid improvement in their hemodynamics with this medicine.
For these patients, you have to first understand how sick they are. For patients in overt shock, then you will probably be reaching for Nipride to help stabilize them and think about those long-term medications later. Otherwise, I would use an ACE/ARB/ARNI unless there a specific clinical reason why the patient can’t be on one.
- What about inotropes that also vasodilate?
The term “inodilators” is often used to describe Mirinone and Dobutamine, but I typically associated it with Milrinone. Milrinone does have a combination of actions when thinking of your hemodynamic parameters. It increases contractility and vasodilates, so you get both increased inotropy and afterload reduction. In comparison, Dobutamine is more of a pure inotrope and does not have as much as the vasodilatory effect as Milrinone. However, we typically are using these medicines primarily for the inotropic effect in the clinical setting, rather than for afterload reduction.
- When adding afterload reducing agents, our goal is to lower the blood pressure. Is there a target blood pressure we are shooting for? How do we know when a patient is not “tolerating” these therapies?
When I treat patients with heart failure, I don’t have a target blood pressure in mind. I usually am most concerned about the blood pressure when it becomes a contraindication to starting or continuing the heart failure medicines that we know provide a great benefit to these patients. Thus, the question becomes; when is the blood pressure too low? I generally answer this question via patient symptoms. If a patient is having symptomatic hypotension, then I will re-evaluate their medication regimen. I get particularly concerned when a patient says they are having consistent pre-syncopal symptoms or lightheadedness, for example. Nevertheless, I think we all have a limit for patients who are asymptomatic. For me, I usually will start to worry when patients have systolic blood pressures in the 70s. I am comfortable with asymptomatic patients with systolic blood pressures in the 80s.
Again, I think blood pressure tells us how much we can give. When you see patients who are hypertensive, then you typically will be able to get them on more of the core therapies of heart failure. This concept is important to explain to patients. Patients are often confused because we are often putting them on these medicines when their blood pressure is already low. So I often tell patients that, “for you, this is not a blood pressure medication, it is a heart medication that will help you live longer, improve your symptoms, and prevent you from going to the hospital”.
Inotropy:
- What is inotropy and what therapies can we use to manipulate it?
Inotropy is basically how strongly the heart can contract, independent of the preload. It is purely a measure of squeezing force.
We typically use Milrinone and Dobutamine to increase this hemodynamic parameter in patients who are very sick. However, we typically are not directly altering inotropy in most heart failure patients. You would think that we should give all heart failure patient’s these medicines if it makes your heart beat stronger, but the data doesn’t tell us that. These medicines don’t improve mortality and may actually worsen patient mortality.
Thus, inotropes are not the way to treat the disturbed hemodynamics of heart failure, unless nothing else is working. For most patients, you will want to optimize preload and afterload before considering inotropes.
- What are the main differences between Dobutamine and Milrinone?
In regard to Dobutamine and Milrinone, we currently don’t really know if one of these medicines is better than the other. In my clinical experience, I often see patients that just do better on one of these medicines without an identifiable reason of why that is so. Some patient’s just feel better on Dobutamine vs. Milrinone, and vice versa. There are also differences in how Cardiologists view these medicines. Some Cardiologists feel Milrinone is truly a better medicine than Dobutamine (i.e. provides more clinical benefit). I am not totally convinced of this, so just understand there is some practice pattern variability to this.
I do think you can run into more problems with Milrinone. The major physiologic difference between Milrinone and Dobutamine (other than their differing mechanism of action), is that milrinone is renally cleared. I would use caution in using Milrinone in patients with significant renal dysfunction as it can accumulate and lead to significant hypotension. Milrinone is also thought to cause more hypotension than Dobutamine, even in patients without renal dysfunction, so that should be a consideration as well. Both inotropes can be arrhythmogenic, which is also important to think about in patients with significant atrial and ventricular disturbances.
Practically speaking, if a patient is sick enough to need an inotrope, then choose the agent you feel most comfortable with the understanding there may be some trial and error, unless there is a specific reason not to use one of the agents (i.e. renal dysfunction).
- Beta blockers are a mainstay of treatment for patients with Heart Failure, however, they have both negative inotropic and chronotropic effects. Can you discuss how you decide when it is safe for patients to receive beta blockers in the inpatient setting? Do you recommend any particular strategy for safe initiation?
I think the most common situation (hopefully) is that patients being admitted to the floor for an acute heart failure exacerbation were already on a beta blocker. I almost always will continue the beta blocker in patients who are clearly “warm” or well perfused, even if they are congested. I will hold or dose reduce the beta blocker if I think the patient is not well perfused or are potentially headed in that direction. Unless there are active arrythmias that we are also treating with a beta-blocker, we need to be thoughtful here as high doses of beta blockers in decompensated systolic heart failure can precipitate cardiogenic shock.
Strictly speaking, initiating a beta blocker is best done when a patient is euvolemic or approaching euvolemia. For patient’s admitted with new onset heart failure and volume overload, it should not be the first medicine that you put them on. Sometimes I will see this medicine started first because it is seen as the “safest” in terms of side effects like renal dysfunction. It really shouldn’t be viewed this way, particularly in patients who have more advanced left ventricular dysfunction. However, starting a beta blocker in the hospital is much safer than starting it as an outpatient. So for these patients where you are initiating GDMT, your goal should be to diurese them to euvolemia and then start the beta blocker.
a. What about metoprolol tartrate?
I don’t use this medicine for the treatment of heart failure. I use metoprolol succinate almost always for these patients. While patients may have other reasons to be on metoprolol tartrate (like atrial fibrillation, assuming doses are given on time), the most important thing is what medicines the patients are discharged with. It should always be metoprolol succinate for the treatment of heart failure.

Leave a comment